




 Pain
Pain



Symptom Management in Palliative Care
In this article, I look at symptom management in palliative care. I describe common symptoms that can occur in patients receiving palliative and end of life care. Finally, I discuss non-pharmacological ways to help manage these, to help reduce polypharmacy and improve patient care and comfort.
 Pain
Pain
Pain is a common symptom in patients receiving end of life and palliative care, and it can be difficult to manage. Strong analgesia may reduce pain, but can have unpleasant side effects including nausea, vomiting, constipation and drowsiness.
Types of pain and their causes include:
- Neuropathic (nerve damage) pain: Causes include cancer, motor neurone disease (MND), multiple sclerosis (MS) and diabetes complications.
- Nociceptive (tissue damage) pain: Caused by trauma, surgery or burns.
- Referred pain: Occurs when there is an injury in one part of the body, but the pain is felt somewhere else. Causes include kidney and liver disease, pancreatitis, heart attack, shingles and fibromyalgia. It happens because the nerves in the body are all part of a large, connected network.
- Phantom pain: Felt from a body part that is no longer there, following amputation.
Breathlessness
Breathlessness is a common symptom, and can be very distressing for the person and their loved ones. Causes include:
- Anxiety
- Infection
- Increased secretions
- End stage COPD
- End stage heart failure
- Lung cancer
- Pulmonary fibrosis
Breathlessness causes anxiety, but equally anxiety can result in worsening breathlessness; an extremely unpleasant vicious circle. Anxiety can also increase due to discomfort, pain, and psychological and social factors.
Audible Secretions
Causes of audible secretions include infection, respiratory pooling, inability to expectorate and organ failure. They can be very distressing for loved ones to witness.
While medication can help to prevent further secretions developing, it is not very effective in reducing secretions already there.
Skin Damage
Because patients at the end of their life are so unwell, they are very vulnerable to skin damage caused by pressure, shear and friction.
Certain diseases which affect the skin can also cause breakdown. Examples include cutaneous T cell lymphoma, graft versus host post stem cell transplant, dermatological conditions, diabetes, and trauma.
As the patient approaches end of life, skin breakdown can occur due to:
- Multiple organ failure (including skin)
- Peripheral shut down
- Hypersensitivity
- Localised reactions from a subcutaneous cannula ‘tissuing’ causing erythema, swelling, tenderness and hardness
Nausea and Vomiting
Nausea and vomiting can be side effects of medication – for example opioid analgesia. They can also be caused by pain and anxiety.
It can be difficult to support a person who is vomiting if they are bedbound and unable to sit up.
Non-Pharmacological Symptom Management in Palliative Care
Often patients become bedbound as they approach last hours to weeks of life. Also, they may decline repositioning because it is too tiring, or because they are uncomfortable or in pain.
Family members may also decline repositioning when a patient is unconscious, for various reasons.
Some patients will remain bedbound for months or even years, due to disease processes such as dementia, stroke, MND, MS and frailty.
With this in mind, how can we help to manage symptoms in these patients, in conjunction with medication?

Positioning
Beds which can profile into a cardiac chair position can benefit a conscious bedbound patient (or someone spending a lot of time in bed). Sitting up in bed can help to:
- Reduce breathlessness, as the chest can expand more than in a supine position.
- Assist with pressure area care, due to the positional change.
- Help the patient to cough more easily, and remove secretions.
- Provide a better, safer position for someone who is vomiting.
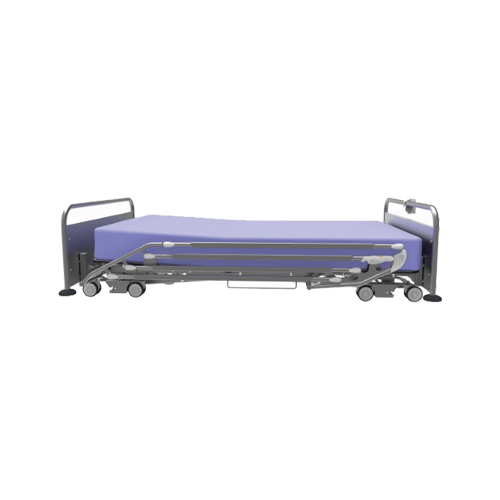
Lateral Tilt
A bed frame like Eleganza 5, which has full platform lateral tilt, can assist with symptom management in several ways:
- Full body lateral tilt helps to mobilise respiratory secretions, helping to reduce pooling and thickening, and making them easier to remove. This can be particularly useful for patients who are unable to sit up in bed.
- Lateral tilt provides off-loading and pressure redistribution, helping with pressure area care.
- A patient at end of life is typically nursed on their back, as repositioning is difficult due to muscle and cognition loss. Lateral tilt may be able to provide comfort to a patient and their loved ones, with better face to face care and interactions.

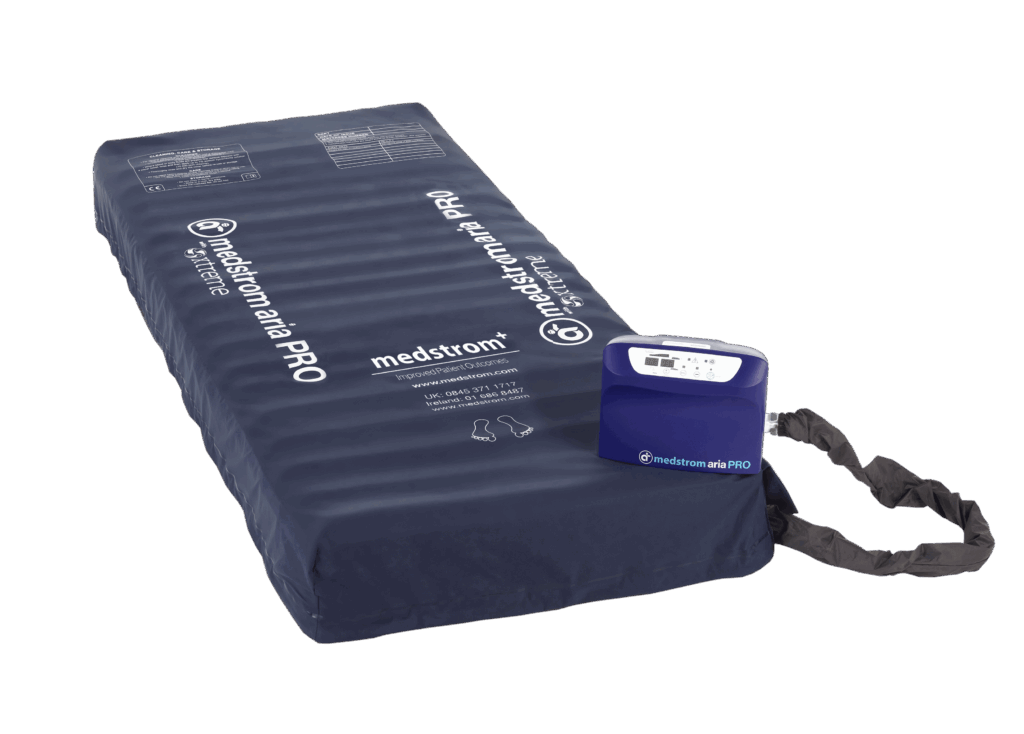
Pressure Area Care
Many palliative and end of life patients are at very high risk of developing skin damage, and where it already exists, deteriorating further. This can happen despite using a dynamic air mattress.
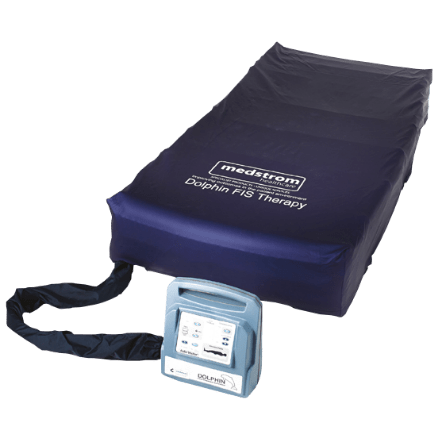
The Dolphin Therapy fluid immersion simulation surface is one of the few viable ‘step up’ options from a dynamic air mattress. Outcomes from over 3,000 patients have shown it is extremely effective at both preventing and treating skin damage in highly complex patients.
The same data demonstrated it improved comfort, pain management and sleep in over 99% of patients, and reduced turning frequency in 98%.
Outcomes for end of life patients specifically have also been analysed, with very similar results.
Case studies have shown using Dolphin Therapy and the Eleganza 5 bed together can give powerful combined benefits. Dolphin Therapy, via better pain management, has also reduced analgesia requirements for some patients.

Summary
In my experience as a Palliative Care Clinical Nurse Specialist, selecting equipment which may help to alleviate symptoms and reduce polypharmacy can often be overlooked. Funding is not always available, and there may be a standard list of products which can be ordered, with no scope to look beyond that.
I’ve now seen first hand how certain products can really help patients receiving palliative and end of life care. While they will not replace medication, they can help to alleviate symptoms and make the person’s quality of life better at an extremely difficult time.